EXPERIENCE: In her recent inaugural lecture, Professor Floretta Bonzaier says women portray themselves as strong and in control of their lives, though deeply limited by intersectional forms of oppression such as gender, race and class…
By Niémah Davids
Women’s stories and their experiences of gender-based violence (GBV) challenge the popular narrative of a passive and helpless woman. Instead, their experiences reveal “counter-stories” that challenge society’s focus on physical violence as the only form of legitimate violence. Women experience psychological abuse as being more harmful than physical abuse.

This was one of the points made by Professor Floretta Boonzaier from the University of Cape Town’s (UCT) Department of Psychology during her recent inaugural lecture titled “Finding hope and healing while researching violence: Decolonial feminist explorations into gender-based violence (GBV) and femicide”. The inaugural lecture coincided with Boonzaier’s 20th year at UCT. For her, to profess as black and as a woman is two interwoven stories: the story of her scholarship and the story of her. She starts the journey of her life with the question: “How was it that this girl from Mitchell’s Plain came to do this work at a place like UCT, where her experiences have vacillated between the extremes of alienation, isolation and exclusion to those of love, of joy, of belonging and of healing?”
Boonzaier said women portray themselves as strong and in control of their lives though deeply limited by the intersectional forms of oppression such as gender, race and class that shape their lives. She said women also use their stories as a form of resistance and empowerment. “Collectively, this work was important for showing how – despite the fact that women survivors of violence often experience shame – women also use their stories as a means for resistance and empowerment, even in the face of economic and other difficulties. They find ways to centre the feminist narrative of resistance against men’s violence,” she said.
Boonzaier said feminism was practised in her home. Though the word was never used, she learned the true meaning of feminism from her mother and some family members. She also learnt feminism from women in the different Cape Flats communities where she lived in Heideveld and Mitchell’s Plain. These women held their families together and displayed massive strength and resilience in the face of state and other forms of violence. These women also ensured that their loved ones were fed, provided shelter and meals to those who were destitute.
“I learned feminism from respected members of these different communities, while doing work underground to support the struggle against apartheid,” she said. Her initial work focused primarily on intimate partner violence. The questions that regularly occupied her mind was society’s obsession with why women stay in abusive relationships.
Every article she read blamed women who stayed with their abusive partners, locating the question of abuse with the abused women rather than with the men who perpetuate that abuse. She then wanted to understand the context in which women in abusive relationships find themselves after suffering violence at the hands of a partner.
Her research found that women find multiple ways to resist violence, and to resist the gendered expectations of them as women.
Her research next focused on how women relay their experiences of violence and abuse, and how these stories shape how they see themselves in the world, opening safe spaces for storytelling aided this process. “Telling stories about the violence they experienced allowed women to represent their inner realities, to interpret their past, to understand their present and to envision their futures,” she said. “Telling stories on their own terms allowed women the opportunity to reclaim their narratives in ways that challenge dominant ideas of what an abused woman is supposed to be.”
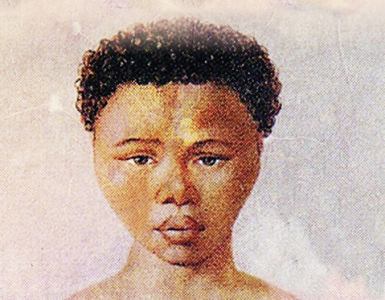
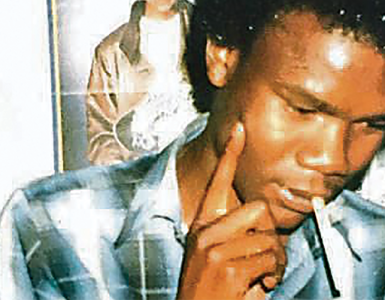
Boonzaier also discussed how the South African media report on GBV and intimate partner violence and highlighted the story of 17-year-old Anene Booysen, who was raped and murdered in Bredasdorp in the Western Cape’s Overberg region. As she went through media reports, she realised that while much had been written about Booysen’s death, the public knew very little about her life.
“All we really knew was the recollection of her movements on the night of the murder and the very graphic details about how she died.” Her research demonstrated that, while reporting on the murder, the media used colonial legacies that “hyper-visiblise” the bodies of black women in the most public ways and yet hid their identities. Her research also showed how the media’s representation of GBV, particularly in the case of Booysen, dehumanised black women “making them less deserving of our empathy”.
“I argued that the ways in which Anene Booysen was represented mirrored the colonial stories about Sarah Baartman,” she said. In concluding her lecture, Boonzaier returned the question she posed at the beginning, and asked: “What does it mean to profess while black and woman?”
“In this moment that I’m owning as a celebration, it’s hard to stand here and not recall the indignities I had to suffer in order for me to be considered full, a full professor. It’s hard not to recall the indignities of what it meant to be racialised as coloured in the apartheid and colonial imageries of fellow students when I was a student here,” she said.
“It’s hard not to recall the snide remarks, forms of surveillance and racism I experienced from colleagues as I worked hard to move up the ranks.” “Here I am, in celebration of this occasion, talking decolonial love, hope and joy. For us, the practice of decolonial feminist psychology has centred radical hope, love and healing – a methodology of decolonial love and a commitment to creating alternatives to the present,” she said. – UCT News
Comment
DISCHARGING AILING BUT FIXABLE SYSTEM
Few will disagree that our health system has been needing serious overhaul for quite some time. That it sorely needs life-support sooner than later, is beyond argument, having not fully recovered from the vagaries of segregated, unequal health system of the apartheid era and later the tinkering of the system by the ANC to no better, in the past 30 years of its rule. The reality is that South Africa is saddled with a two-tiered, and highly unequal, healthcare system – with a state-funded public sector catering to the majority – 71 percent – of the population. On the other hand, the private sector that is largely funded through individual contributions to medical aid schemes or health insurance serves around 27 percent of the population.
Sadly, the public sector is underfunded while most South Africans can’t afford the exorbitant cost of private care. To balance the scales, the National Health Insurance Scheme (NHI) is running a gauntlet of unrelenting opposition – a noble idea, but currently causing much consternation at the middle-class dinner tables. For its part, NHI seeks to provide universal healthcare by buying services from health professionals to be delivered at private and public facilities. But there are still many doubts about whether NHI is the panacea to the country’s enduring healthcare challenges.
From the look of things, it would seem the NHI – much-needed as it is to redress historical imbalances in our society – may compound rather than alleviate problems in the long term. In 2021, Russell Rensburg, the director of the Rural Health Advocacy Project, raised some pertinent points about the prognosis for the NHI. His observations, made in the midst of the Covid-19 at the time, precipitated a seminal question at the time: What has the pandemic exposed about South Africa’s healthcare system?
His answer was rather illuminating and duly raised the further questions that have lingered over the years, about how to definitively fix our healthcare system so that South Africa can achieve or perhaps make a significant dent to the World Health Organization (WHO) universal coverage goals. Firstly, Rensburg pointed out, South Africa’s biggest problem is that the health needs of its people exceed capacity. Secondly, the vast majority of people actually don’t know their health status which may delay access to care, he says. And, thirdly, the way the system is funded perpetuates inequality.
A fourth point, not raised by Rensburg but yours truly: the flagrant mismanagement of scarce healthcare resources deployed from the strained national purse every year, to no great effect. Indeed, there are no simple solutions to South Africa’s health crisis, but, as Rensburg points out, we have a once-a-generation opportunity to begin addressing the crisis. “The country has to find a way to make sure the availability of care is spread more evenly throughout the system. We can’t look at the private and public sectors separately. One has an impact on the other,” says Rensburg.
In addition, South Africa’s healthcare system is inefficient – both public and private, he argues. The cost of healthcare is too high as well – a reality that riles even Health Minister Aaron Motsoaledi. Yet, in the long term, the imperative to improve the quality of care in the public sector should help balance out people’s need to have expensive medical insurance.