ROLL-OUT: A near-100% effective HIV prevention injection is expanding rapidly across Africa — but geopolitical tensions, funding gaps and policy choices could determine who truly benefits…
By Kerry Cullinan and WSAM Reporter
A groundbreaking HIV prevention drug hailed as a potential “endgame” in the fight against the epidemic is expanding across Africa — but for South Africa and the continent at large, access will be shaped as much by politics and policy as by science.
The United States and the Global Fund have announced a major scale-up of lenacapavir, a twice-yearly injectable drug that is nearly 100% effective in preventing HIV transmission. The revised commitment will now reach up to three million people globally — a million more than initially planned — with Africa firmly at the centre of the rollout.
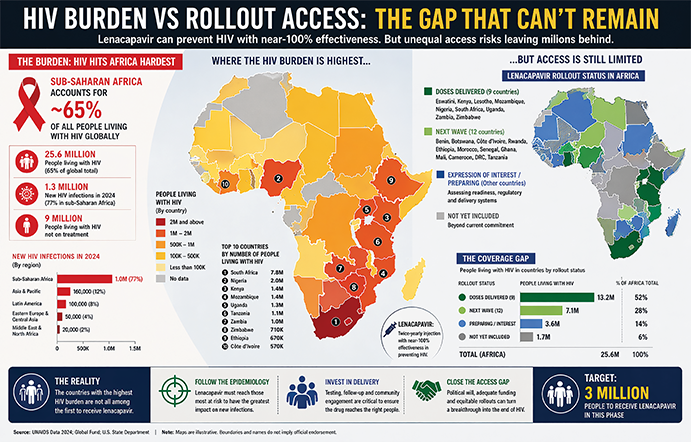
For a region that still carries the heaviest burden of HIV, the implications are enormous. Sub-Saharan Africa accounts for the vast majority of the world’s 1.3 million new HIV infections annually, while an estimated 41 million people globally are living with the virus.
We have a tool that can stop HIV in its tracks — the real
test is whether Africa gets it fast enough, and fairly enough…
The promise of lenacapavir lies not only in its effectiveness, but in its simplicity. Unlike daily pills, it requires just two injections a year — a shift that could dramatically improve adherence, particularly among vulnerable and mobile populations.
Africa first — but not equally
Since November last year, around 135 000 doses have already been delivered to nine African countries: Eswatini, Kenya, Lesotho, Mozambique, Nigeria, South Africa, Uganda, Zambia and Zimbabwe. Eswatini led the way as the first country globally to receive the drug, highlighting how Africa is increasingly becoming the frontline for cutting-edge HIV interventions.
Twelve more countries — including Rwanda and Morocco — are expected to follow, with the Global Fund targeting 24 countries by 2027.
But this is not a blanket rollout. Access is being prioritised for countries that can demonstrate readiness — including the ability to test patients, enrol HIV-negative individuals and ensure follow-up injections after six months.
That requirement exposes a persistent fault line: while the science may be universal, health system capacity is not.
SA’s paradox
For South Africa — home to the largest HIV-positive population in the world — the rollout presents both opportunity and contradiction.
On one hand, the country is among the early recipients of lenacapavir doses, reinforcing its central role in the global HIV response.
On the other, it has not been included in the United States’ bilateral Memorandums of Understanding (MOUs), which are helping to fast-track access and funding in other high-burden countries.
The exclusion is widely linked to broader political tensions between Washington and Pretoria.
That leaves South Africa navigating a more complex path — relying on multilateral channels, domestic funding and partnerships, rather than direct US bilateral support.
Yet, even without an MOU, the arrival of lenacapavir in the country has been framed as a sign of “commercial diplomacy” between the two nations — a reminder that science and politics remain deeply intertwined.
Who gets the drug?
Beyond supply, the bigger question is who will actually receive lenacapavir. Public health experts have long identified “key populations” — including sex workers, men who have sex with men, people who inject drugs, and adolescent girls — as those most at risk.
However, shifting political priorities, particularly from the United States, are narrowing that focus. Current US policy is placing strong emphasis on preventing mother-to-child transmission, prioritising pregnant women and children.
While this is a critical goal, it risks sidelining other high-risk groups that drive new infections across Africa. Global Fund leadership has signalled a broader approach, emphasising the need to “follow the epidemiology” and ensure the drug reaches those most at risk — even where governments may be reluctant. This tension — between public health evidence and political priorities — could ultimately determine the impact of lenacapavir.
Race for generics
Another key factor for Africa will be affordability and long-term supply.
In a move widely welcomed by global health advocates, Gilead Sciences — the US company behind lenacapavir — has already signed royalty-free agreements with six generic manufacturers.
The first generic versions are expected by mid-2027, a development that could significantly lower costs and expand access across lower-income countries. The Global Fund has also issued a call to manufacturers to accelerate production, aiming to ensure that supply keeps pace with demand. But even here, time is critical.
Every delay means more infections — and Africa cannot afford a repeat of past rollouts where life-saving drugs took years to reach those who needed them most.
A turning point
For decades, the fight against HIV has been defined by incremental progress: better treatment, improved prevention, and stronger awareness.
Lenacapavir changes that equation.
It offers, for the first time, a realistic pathway to dramatically reducing new infections — potentially bending the curve of the epidemic in Africa within a generation.
But the science alone will not end HIV. Success will depend on whether African governments invest in delivery systems, whether communities are meaningfully included, and whether global partners align funding with real-world risk.
It will also depend on whether countries like South Africa — with the scale, expertise and burden — can leverage this moment despite geopolitical headwinds.
The drug may be a medical breakthrough. Turning it into a public health victory will require something far more difficult: coordination, urgency and political will. – Health Policy Watch/WSAM
5 THINGS TO KNOW
LENACAPAVIR: THE BASICS
1. Near 100% protection
Clinical trials show the injection is almost completely effective at preventing HIV.
2. Twice a year
Just two injections annually — a major shift from daily prevention pills.
3. Africa at the centre
First doses already delivered to nine African countries, including South Africa.
4. 3 million target
US and Global Fund aim to reach three million people in the next phase.
5. Generics coming
Cheaper versions expected from 2027 to expand access across the continent.



























